When the Liver Fails the Brain: Hepatic Encephalopathy in Dogs & Cats
- Dr Andrew Matole, BVetMed, MSc

- 10 hours ago
- 10 min read
What Is Hepatic Encephalopathy?
Consider your pet’s liver as the body’s main chemical processing plant — it handles all substances absorbed from the gut and transforms toxic ammonia into safe urea for elimination via the kidneys. (Häussinger & Görg, 2010; Lidbury et al., 2016) If this process is disrupted, due to liver disease or an abnormal bypass vessel, ammonia builds up and can eventually affect the brain.
Hepatic encephalopathy (HE) is a neurological syndrome that arises as a consequence of liver dysfunction. (Lidbury et al., 2016) Importantly, it is not a primary brain disorder—often, the brain remains structurally normal, but it is affected by toxins that the compromised liver can no longer eliminate. This distinction is crucial because it indicates that the condition can potentially be reversed with proper treatment. (Rothuizen, 2009)
HE is most commonly observed in young dogs and cats with congenital portosystemic shunts (cPSS), as noted by Berent & Tobias (2009). It can also develop in older animals suffering from chronic liver diseases such as hepatitis and cirrhosis and, particularly in cats, hepatic lipidosis (Armstrong & Blanchard, 2009). Data from studies show that HE complicates the clinical course in about 50–70% of dogs diagnosed with cPSS (Tivers et al., 2014).
Key Clinical Point
HE usually occurs in episodes rather than as a continuous condition (Lidbury et al., 2016). Signs can come and go as blood ammonia levels change. A key diagnostic feature is post-prandial exacerbation, particularly after high-protein meals. Many owners report their pet having “funny turns"—appearing entirely normal between episodes.
The Liver: Normal Anatomy & Blood Supply
The liver is the largest internal organ in dogs and cats, located just behind the diaphragm in the upper right abdomen. Its unique dual blood supply forms the basis of hepatic encephalopathy (HE) pathology (Nelson & Couto, 2014):
The hepatic artery provides oxygen-rich blood from the aorta (~25% of hepatic blood flow).
The portal vein supplies nutrient- and toxin-rich blood from the gastrointestinal tract (~75% of hepatic blood flow), including ammonia produced from colonic bacterial protein metabolism (Häussinger & Görg, 2010).
In healthy animals, the portal vein transports ammonia directly to hepatocytes, where it is detoxified within seconds via the urea cycle (Bosoi & Rose, 2009; Häussinger & Görg, 2010). If this pathway is disrupted—due to structural shunting or liver cell damage—hepatic encephalopathy occurs.
How HE Happens — The Ammonia Cascade
HE is a syndrome with multiple contributing factors, but its primary mechanism involves the buildup of neurotoxins originating from the gut—mainly ammonia (NH₃/NH₄⁺)—in the systemic circulation (Häussinger & Görg, 2010; Lidbury et al., 2016). Under normal circumstances, the portal vein transports colonic ammonia to hepatocytes within seconds, where it is transformed into urea through the urea cycle. This swift detoxification process fails when portal blood bypasses the liver (PSS) or when the hepatocellular mass is critically reduced (Bosoi & Rose, 2009; Häussinger & Görg, 2010).
Beyond Ammonia: The Neuroinflammation Pathway
Ammonia levels alone do not accurately predict the severity of clinical HE. Tivers et al. (2014) showed that combining hyperammonaemia with systemic inflammatory response syndrome (SIRS) provides a much better prediction of HE presence than ammonia alone. Pro-inflammatory cytokines, such as interleukin-6 (IL-6) and tumour necrosis factor-α (TNF-α), enhance ammonia-induced astrocyte dysfunction (Gow et al., 2012). Manganese buildup due to impaired liver excretion disrupts dopaminergic pathways (Gow et al., 2010), while the enhancement of GABA-A receptor activity by neurosteroids contributes to the sedation and obtundation seen in advanced HE (Schafer & Jones, 1982).
What Causes HE in Dogs & Cats?
Any condition that substantially diminishes the detoxification capacity of the liver can precipitate HE (Lidbury et al., 2016; Rothuizen, 2009). The two primary categories are portosystemic vascular anomalies (abnormal vessels bypassing the liver) and hepatocellular disease (damage to liver cells leading to decreased functional hepatic mass) (Berent & Tobias, 2009).
Portosystemic Shunts (PSS) – Most Common in Young Animals
Portosystemic shunts are abnormal vascular communications between the portal and systemic venous circulations, either congenital or acquired secondary to portal hypertension. (Berent & Tobias, 2009) Congenital shunts result in an atrophied and under-developed liver (microhepatica) due to chronic deprivation of portal flow. (Berent & Tobias, 2009; Tivers & Lipscomb, 2018) Acquired multiple extrahepatic PSS (AMEPSS) are a consequence of sustained portal hypertension from chronic progressive hepatic disease. (Rothuizen, 2009)
Hepatocellular Disease – More Common in Older Animals
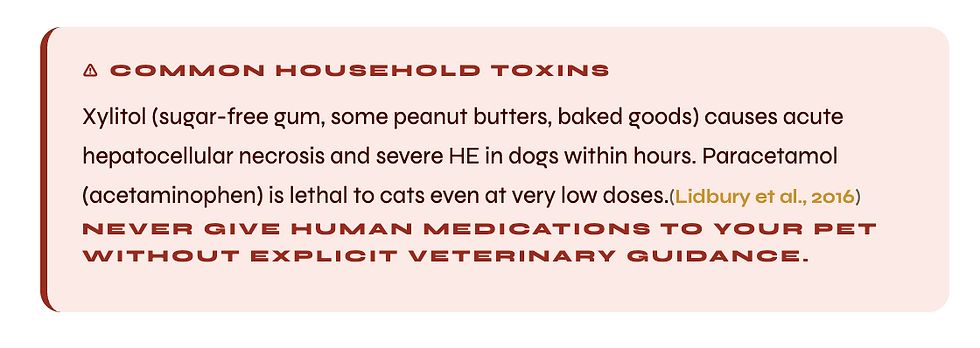
In chronic hepatitis, cirrhosis and hepatic lipidosis, functional hepatocyte mass is reduced below the threshold level required for adequate ammonia detoxification (Armstrong & Blanchard, 2009; Rothuizen, 2009). Within hours of ingestion of xylitol, Amanita mushroom toxins or paracetamol (acetaminophen), which can cause acute toxic hepatic necrosis, fulminant HE can be precipitated (Lidbury et al., 2016).

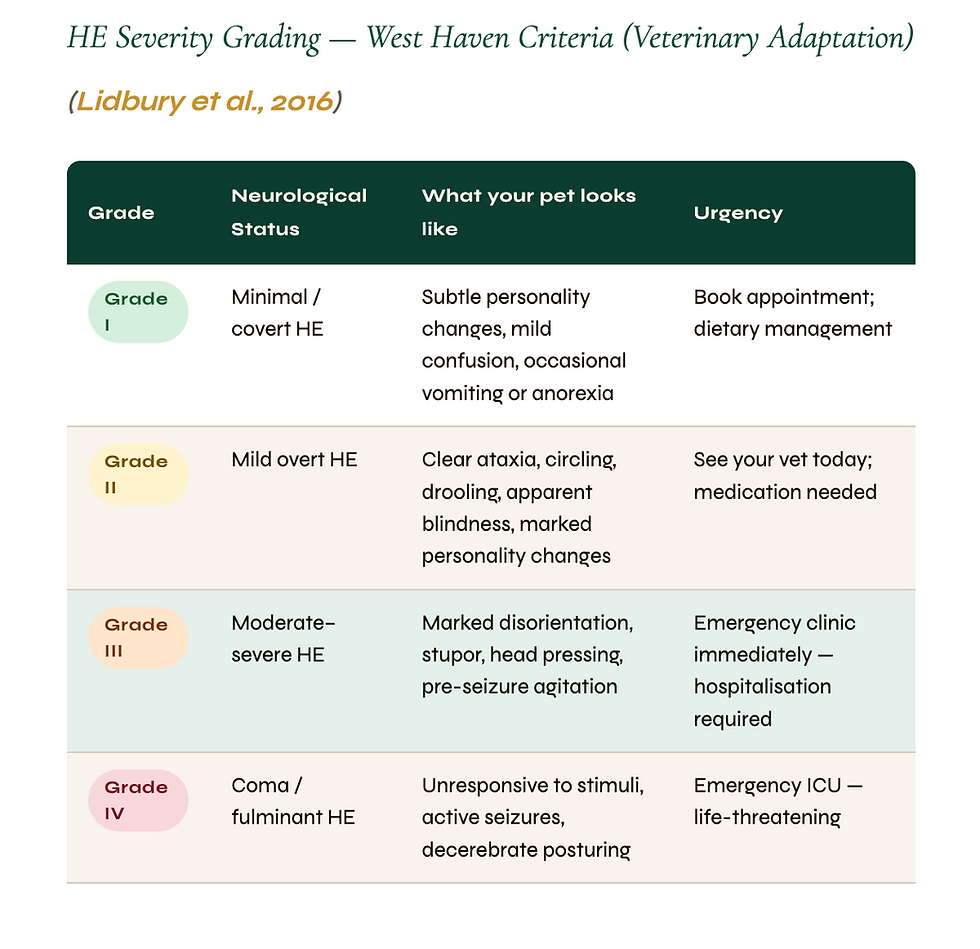
Recognising HE – Clinical Signs
HE clinical signs are protean and episodic and are often exacerbated post-prandially (after high-protein meals) (Lidbury et al., 2016; Nelson & Couto, 2014). Signs can be as subtle as behavioural changes (Grade I) or as severe as seizures and coma (Grade IV). A hallmark diagnostic feature is the episodic nature, and owners should seek veterinary assessment even after complete apparent recovery (Lidbury et al., 2016).
“Head pressing – where an animal persistently pushes their head against a wall or floor – is one of the most dramatic and distinctive signs of hepatic encephalopathy. Any episode of head pressing must be seen by a veterinarian on the same day.”


Tests & Imaging for Diagnosing HE
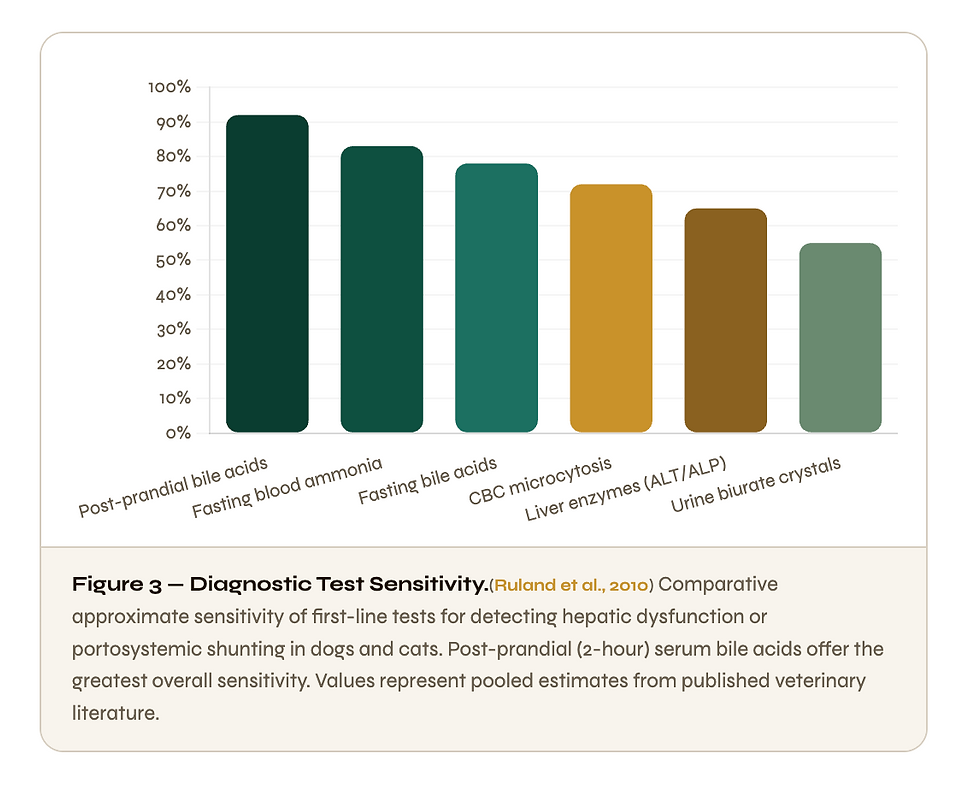
The diagnosis of HE requires the integration of clinical presentation, signalment (breed and age), biochemical findings and advanced imaging (Lidbury et al., 2016; Ruland et al., 2010). No single test is diagnostic. The systematic approach begins with a clinicopathological assessment, then imaging, and to confirm the diagnosis, CT angiography (Ruland et al., 2010).
Blood & Urine Analysis
Blood ammonia: Levels >100 µmol/L (normal <50 µmol/L) are strongly indicative of portosystemic shunting or hepatic failure (Ruland et al., 2010). Samples should be analysed on ice within 30 min of collection, as ammonia is highly temperature sensitive and prone to artefactual elevation. False positives are common in cats. The test of choice is bile acid testing (Ruland et al., 2010).
Serum bile acids (SBA): Pre-prandial and 2-hour post-prandial SBA is the most sensitive marker of hepatic portal blood flow. Ruland et al. (2010) reported a sensitivity of 92% for postprandial SBA in the detection of PSS (Ruland et al., 2010). Postprandial values >25 µmol/L (dogs) and >20 µmol/L (cats) are suggestive of significant hepatic dysfunction, even if standard liver enzyme activities are normal.
Haematology: Microcytosis (small red blood cells without anaemia) is a typical finding in dogs with congenital PSS, secondary to reduced hepatic blood flow and reflecting altered iron metabolism (Berent & Tobias, 2009). Common biochemical findings are hypoalbuminaemia, hypocholesterolaemia, low BUN and hypoglycaemia (Nelson and Couto, 2014).
Urine: Examination of urine sediment for ammonium biurate crystals is an almost pathognomonic finding for portosystemic shunting (Berent & Tobias, 2009) and may be seen before any other laboratory abnormality is evident.
Diagnostic Imaging
Diagnosis of PSS is primarily based on abdominal ultrasonography with a sensitivity of 74–95% for detection of shunt vessels in experienced hands (Berent & Tobias 2009). Doppler ultrasonography can be used to assess the direction and velocity of portal blood flow. Computed tomographic angiography provides the gold standard for definitive anatomical shunt characterisation prior to surgery, providing accurate three-dimensional vascular mapping which is critical for surgical planning (Tivers & Lipscomb, 2018). Nuclear scintigraphy (trans-splenic portal scintigraphy) offers a non-invasive quantification of the portosystemic shunt fraction (Berent & Tobias 2009)
Treatment — Stabilise, Then Heal
The management of HE is biphasic:
(1) immediate crisis stabilisation of the acutely ill patient and
(2) definitive control of the underlying cause where possible (Lidbury et al., 2016; Tivers & Lipscomb, 2018).
The best long-term options for a cure for congenital PSS are surgery or interventional radiology (Tivers & Lipscomb, 2018).



Prognosis – What To Expect
Prognosis depends mainly on the underlying aetiology and the speed of starting treatment. The most frequent cause of congenital PSS is good results with surgical correction. (Lidbury et al., 2016; Tivers & Lipscomb, 2018) Animals with HE secondary to advanced irreversible fibrosis have a more guarded prognosis, but quality of life can be excellent with appropriate ongoing medical management. (Rothuizen, 2009)
With successful surgical management of extrahepatic PSS, dogs have a median survival of >10 years, with most not requiring ongoing hepatic medication. (Tivers & Lipscomb, 2018). Primary perioperative risks are post-attenuation seizures (5–8%), acute portal hypertension and anaesthetic complications, all of which are manageable in experienced hands. (Lidbury et al., 2016; Tivers & Lipscomb, 2018)
Cats with hepatic lipidosis have an excellent prognosis (60-80% survival) if aggressive nutritional support is started early (Armstrong & Blanchard, 2009), usually via oesophagostomy or percutaneous endoscopic gastrostomy (PEG) tube feeding.
Frequently Asked Questions
My dog had a circling fit but is back to normal. Should I still take him to the vet?
Yes, it is important to contact your vet promptly even if there seems to be a complete recovery. Episodic neurological symptoms that completely resolve are characteristic of HE, due to blood ammonia levels varying throughout the day (Lidbury et al., 2016). The root liver issue remains unresolved. Tests such as blood ammonia levels, bile acid tests, and abdominal ultrasounds can detect a portosystemic shunt or liver disease before the next — possibly more severe — episode occurs (Ruland et al., 2010).
Is HE curable or is it a lifelong condition?
For animals with a congenital portosystemic shunt, surgical correction can be curative — most dogs who undergo surgery need no further medication or special diet after recovery and can lead completely normal lives (Tivers & Lipscomb, 2018). For animals with acquired hepatic disease, HE can be effectively managed long-term with the right diet and medication (Rothuizen, 2009).
Is it safe to have surgery when my pet has liver disease?
Your pet will be medically stabilised prior to any surgery being considered. In animals with hepatic disease, anaesthetic protocols are based on agents with minimal hepatic metabolism. The perioperative mortality for surgery for extrahepatic PSS at centres of expertise is <8% (Tivers & Lipscomb, 2018). In selected patients, the surgical risk is often much lower than the risk of not operating (recurrent HE crises, progressive liver atrophy and ammonium urolith complications).
What should I feed my pet with hepatic encephalopathy?
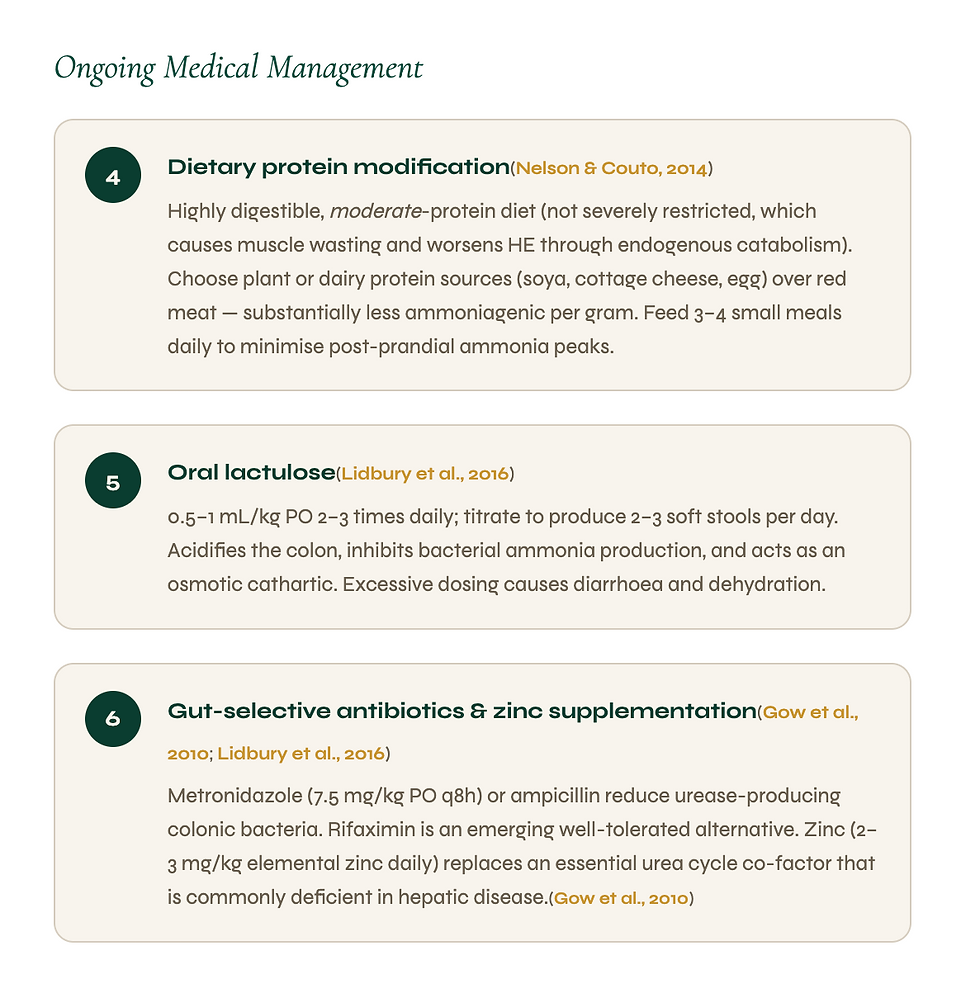
Very digestible moderate protein diet ( not severely protein restricted as this causes muscle wasting and actually worsens HE ) (Nelson & Couto, 2014). Select diets with soya, dairy or egg protein instead of red meat as they produce much less ammonia per gramme during the digestive process. 3–4 small meals daily are advised to decrease post-prandial ammonia spikes.
My cat has not eaten for 3 days and is now drooling and confused. Could this be HE?
This is a medical emergency – contact your vet or emergency clinic immediately. This presentation is very consistent with hepatic lipidosis and secondary HE (Armstrong & Blanchard, 2009). Overweight cats can develop rapid and severe fatty infiltration of the liver if they stop eating for 48 to 72 hours. Ptyalism (drooling) is a classic early sign of HE in cats only (Armstrong & Blanchard, 2009). Affected cats can recover completely with prompt aggressive nutritional support in 60-80% of cases.
Which dog breeds are most at risk of portosystemic shunts?
Extrahepatic PSS is much more common in small and toy breeds, particularly Yorkshire Terriers, Maltese, Shih Tzus, Miniature Schnauzers, and Pugs. Intrahepatic PSS is more common in large breeds such as Irish Wolfhounds, Labrador Retrievers, Golden Retrievers and Australian Cattle Dogs (Berent & Tobias 2009). If you have one of these breeds, discuss liver screening with your vet, especially if your pet seems small for their age, drinks a lot or has had unexplained neurological episodes.
Can I administer lactulose at home during an episode of HE?
If your pet has been prescribed oral lactulose and is showing early mild signs (Grade I – II), your vet may have given you specific instructions on an additional dose at home as a first response (Lidbury et al., 2017). Even if they seem to be improving, always contact your vet. Grade III-IV episodes with seizures, unresponsiveness or severe disorientation should be treated as an emergency veterinary situation immediately.
How do I know if my pet’s liver condition is deteriorating over time?
The best way to detect it early is regular monitoring blood tests (ammonia, paired bile acids, albumin, and liver enzymes) every 3-6 months (Ruland et al., 2010; Lidbury et al., 2016). Warning signs at home include worsening or more frequent HE episodes; new fluid in the abdomen (ascites); progressive weight loss; jaundice (yellow gums, skin, or sclera); or a sudden drop in energy or appetite. Any of these are reasons to see a veterinarian urgently (Rothuizen, 2009).
References
Armstrong PJ, Blanchard G. Hepatic lipidosis in cats. Vet Clin North Am Small Anim Pract. 2009;39(3):599–616.
Berent AC, Tobias KM. Portosystemic vascular anomalies. Vet Clin North Am Small Anim Pract. 2009;39(3):513–541.
Bosoi CR, Rose CF. Identifying the direct effects of ammonia on the brain. Metab Brain Dis. 2009;24(1):95–102.
Congenital portosystemic shunts in dogs and cats: Classification, pathophysiology, clinical presentation and diagnosis. Veterinary Sciences, 10(2), 160. https://doi.org/10.3390/vetsci10020160
Gow, A. G. (2017). Hepatic encephalopathy. Veterinary Clinics of North America: Small Animal Practice, 47(3), 585–599. https://doi.org/10.1016/j.cvsm.2016.11.008
Konstantinidis, A.curable, O., Patsikas, M. N., Papazoglou, L. G., & Adamama-Moraitou, K. K. (2023).
Gow AG, Marques AIC, Yool DA, et al. Whole blood manganese concentrations in dogs with congenital portosystemic shunts. J Vet Intern Med. 2010;24(1):90–96.
Gow AG, Marques AIC, Yool DA, et al. Dogs with congenital portosystemic shunting and hepatic encephalopathy have higher serum concentrations of interleukin-6 than healthy controls. Vet J. 2012;193(1):269–271
Häussinger D, Görg B. Interaction of astrocytes and neurons in ammonia metabolism and hepatic encephalopathy. J Clin Exp Hepatol. 2010;0(1):8–14.
Liatis, T., Lowrie, M., Frowde, P., & Garosi, L. (2024). Tremors in cats with hepatic encephalopathy–congenital portosystemic shunts. Journal of Veterinary Internal Medicine.
Lidbury, J. A., & Steiner, J. M. (2016). Hepatic encephalopathy in dogs and cats. Journal of Veterinary Emergency and Critical Care, 26(4), 471–487. https://doi.org/10.1111/vec.12473
Maddison, J. E. (1992). Hepatic encephalopathy: Current concepts of the pathogenesis. Journal of Veterinary Internal Medicine, 6(6), 341–353.
Nelson RW, Couto CG. Small Animal Internal Medicine. 5th ed. Elsevier; 2014:569–608.
Rothuizen J. Important clinical syndromes associated with liver disease. Vet Clin North Am Small Anim Pract. 2009;39(3):419–437.
Ruland K, Fischer A, Hartmann K. Sensitivity and specificity of fasting ammonia and serum bile acids in the diagnosis of portosystemic shunts in dogs and cats. Vet Clin Pathol. 2010;39(1):57–64.
Schafer DF, Jones EA. Hepatic encephalopathy and the gamma-aminobutyric acid neurotransmitter system. Lancet. 1982;319(8262):18–20.
Stockman, J. (2025). Nutritional management considerations in dogs and cats with hepatic disease. Veterinary Clinics of North America: Small Animal Practice.
Taboada, J., & Dimski, D. S. (1995). Hepatic encephalopathy: Clinical signs, pathogenesis, and treatment. Veterinary Clinics of North America: Small Animal Practice, 25(2), 337–355.
Tivers, M. S., Lipscomb, V. J., & Brockman, D. J. (2011). Congenital portosystemic shunts in cats: Investigation, diagnosis and stabilisation. Journal of Feline Medicine and Surgery, 13(3), 173–184.
Tivers MS, Handel I, Gow AG, Lipscomb VJ, Jalan R, Mellanby RJ. Hyperammonemia and systemic inflammatory response syndrome predicts presence of hepatic encephalopathy in dogs with congenital portosystemic shunts. PLoS ONE. 2014;9(5):e98203.
Tivers MS, Lipscomb VJ. Congenital extrahepatic portosystemic shunts in dogs and cats: treatment and outcome. Vet Clin North Am Small Anim Pract. 2018;48(5):793–818.
Webster, C. R. L., Center, S. A., Cullen, J. M., Penninck, D. G., Richter, K. P., Twedt, D. C., & Watson, P. J. (2019). ACVIM consensus statement on the diagnosis and treatment of chronic hepatitis in dogs. Journal of Veterinary Internal Medicine, 33(3), 1173–1200. https://doi.org/10.1111/jvim.15467
Weingarten, M. A., & Sande, A. A. (2015). Acute liver failure in dogs and cats. Journal of Veterinary Emergency and Critical Care, 25(4), 455–473.


Comments