What is a Cranial Cruciate Ligament Rupture (CrCLR) in the dog?
- Dr Andrew Matole, BVetMed, MSc
- Jan 30, 2022
- 6 min read
Updated: Oct 5, 2022

Cranial cruciate ligament rupture (CrCLR) refers to an extremely common hindlimb lameness in dogs caused by the damage of one of the ligaments that maintain the integrity of the stifle (knee) joint. It can present as an acute hindlimb lameness or acute deterioration of a more chronic problem. Typically it can be a complete or partial, rupture of the cranial cruciate ligament, categorised according to the cause and onset (A, B, C).
Groups A and B Group C
1. Acute onset hindlimb lameness. 1. More insidious development of lameness.
2. Non-weight-bearing initially. 2. Partial tears become complete.
3. Toe-touching starts in 7-10 days. 3. Intact meniscus becomes injured.
4. Limb use improves with time. 4. Other joint problems, e.g., patellar luxation
5. Variable atrophy of quadriceps
muscle groups.











Usually, it happens either as a complete or partial cranial cruciate ligament rupture. It is a condition that is primarily underdiagnosed in many canine patients. CrCLR leads to osteoarthritis (OA) of the joint secondary to the ligament rupture and progresses rapidly if the stifle (knee) joint is not stabilised quickly.

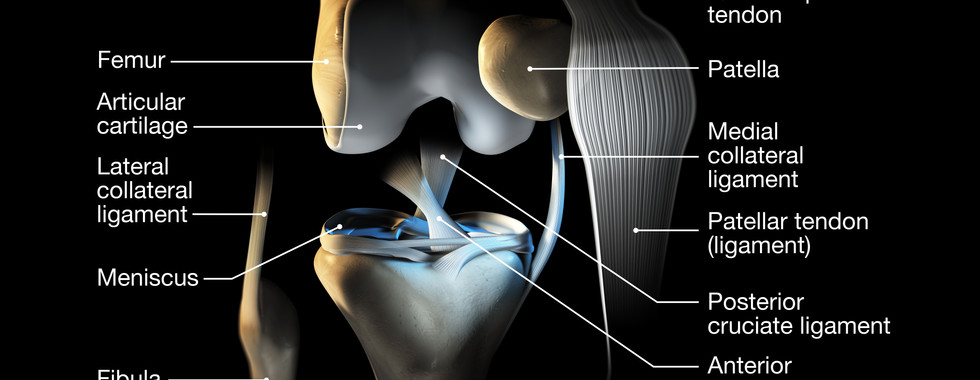
What is the function of the cranial cruciate ligament?

The cranial cruciate ligament (CrCL) or the anterior cruciate ligament (ACL) has an essential biomechanical function as a stabiliser inside the dog knee (stifle) joint, the middle joint in the back leg.

The ligament limits forward movement of the tibia (shin bone) in relation to the femur (thigh) during weight-bearing, internal rotation of the tibia (shin bone), and hyperextension of the stifle(knee joint). The cranial cruciate ligament (CrCL) fine-tunes and guides the stifle through rolling and sliding motions. The ligament has a complex architecture, with distinct geographic regions that have different functional roles depending on the angle and loading conditions.
Causes cranial cruciate ligament rupture (CrCLR).
Though the rupture of the cranial cruciate ligament (CrCL) is mainly a result of slipping, twisting, falling or jumping off furniture, the CrCL ruptures due to chronic joint degeneration due to the weakening of the fibres within the ligament. The cause of the slow deterioration of the cruciate ligament is unknown; however, a subclinical bacterial influence is hypothesised to be the cause. CrCLR occurs less commonly as a classic acute rupture after trauma, and many dogs with unilateral CrCLR subsequently rupture the opposite cranial cruciate ligament over their lifetime.
Trauma-induced rupture of the CrCL results in knee instability and is often supplemented by a sudden non-weight bearing lameness. The other factors include:-
Conformational defects (straight-legged dogs)
Sporting or working dogs,
Hormonal imbalance,
Specific inflammatory conditions of the joints
Underlying systemic disease,
Uncertain (idiopathic).
Senile degeneration (aging)/normal wear/tear.
Immune-mediated diseases, and
Genetic Implications as Cranial Cruciate Ligament Rupture (CrCLR) may be a recessive heritable disease.
What is the prevalence of CrCLR?
Dogs are the most affected by cranial cruciate ligament rupture in companion animals. Large-breed dogs have an increased incidence with the following breeds mostly predilected:-
Labrador retrievers,
Rottweilers,
Bullmastiffs, and
Chow chows
Chesapeake Bay Retriever
Golden retriever
Nova scotia duck tolling













CrCLR mainly occurs in skeletally mature dogs, increasing in middle-aged and older dogs, between 5 and 7 years of age. Skeletally immature dogs rarely have CrCLR, and if it does happen it is only with external trauma.
CrCLR is also more prevalent in females, and sterilised dogs of both sexes are at a higher risk than intact dogs because of the tendency to gain weight.
How does CrCLR present clinically?
Dogs with CCLR usually have a history of acute lameness for several days that improves but then recurs 4 to 6 weeks later and worsens. By the time of initial diagnosis, bilateral rupture is present.
Clinically, the signs include:-
Lameness,
Pain,
The joint is swollen,
Effusion,
Crepitation,
Excessive cranial laxity of the proximal tibia relative to the distal femur (drawer sign, or positive compression test), and
Increased internal tibial rotation.

In chronic injuries, X-rays usually reveal joint effusion and signs of degenerative joint disease. When examined physically, the stifle (knee) joint is swollen and painful upon palpation and during the range of motion tests. During the physical examination, joint friction may be felt with a medial thickening or "buttress" over the upper and medial aspect of the tibia (shin bone), being the standard and confirmatory sign for CrCLR. Laxity of the stifle (knee) joint can also be detected by cranial (forward) drawer or cranial (forward) tibial (shin) bone thrust procedures.
How is CrCLR diagnosed?
Diagnosis of CCLR is based entirely on a history of lameness and knee joint laxity found on the positive cranial drawer reflex test or cranial tibial thrust or by the palpation of the medial buttress. Medial "buttress" occurs rapidly after ligament rupture and is ample indication for surgical joint exploration even in the absence of laxity.
NB: Medial buttress is a firm swelling palpable (felt) on the medial aspect of the proximal (upper) tibia (shin bone); the presence of medial buttress is a characteristic clinical sign of CrCLR. Download the CrCLR diagnostic tree below
How is Cranial Cruciate Ligament Rupture Treated?
The best treatment for CCLR is surgical, for both large- and small-breed dogs, otherwise, 81% to 100% of large-breed dogs remain lame. Medical should be considered ancillary to surgery. Medical therapy without surgery results in the progression of osteoarthritis (OA) and lameness in affected dogs. Non-steroidal anti-inflammatory drugs (NSAIDs) are used to alleviate patient discomfort, given postoperatively as needed for analgesia and continued for pain relief from osteoarthritis (OA). The anti-inflammatory medications (non-steroidal) of choice include Carprofen (Rimadyl), Deracoxib, Meloxicam and Firocoxib.





Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Narcotic analgesics (painkillers) are administered in animals with refractory pain only. Other joint supplements or treatments, such as polysulfated glycosaminoglycans, glucosamine, chondroitin sulfate, milk proteins, pentosan polysulfate, or magnesium, are less consistently beneficial. Corticosteroids are contraindicated in canine osteoarthritis (OA).

After a surgical procedure, activity should be restricted to cage rest for at least 8 weeks.

Limited leash-walking or controlled underwater treadmill physical therapy may hasten functional recovery. swimming, passive range of motion exercises, controlled leash walks, sit-stand exercises, weight shifting exercises, cold therapy, hill walking exercises improve recovery by preventing muscle wasting and increasing joint range of motion.
Weight loss to lean body condition is recommended to reduce stress on the affected leg and protect the unaffected limb from rupture. Animals with secondary osteoarthritis (OA) of the stifle should be placed on high omega-3 fatty acid diets or dietary supplementation to improve clinical signs and decrease the inflammatory processes.






Dietary supplementation and omega fatty acids
How is Cranial Cruciate Ligament Rupture Prevented?
The only known way to prevent CCLR is the maintenance of lean body weight in large-breed sporting or working dogs.
References
de Rooster, H., de Bruin, T., & van Bree, H. (2006). Morphologic and functional features of the canine cruciate ligaments. Veterinary surgery: VS, 35(8), 769–780. https://doi.org/10.1111/j.1532-950X.2006.00221.x
Hayashi K, Manley P A & Muir P (2004) Cranial Cruciate Ligament Pathophysiology in Dogs With Cruciate Disease: A Review. J Am Anim Hosp Assoc 40 (5), 385-390 PubMed.
Marsolais G S (2002) Effects of postoperative rehabilitation on limb function after cranial cruciate ligament repair in dogs. J Am Vet Med Assoc 220 (9), 1325-1330 PubMed.
Wilke V L et al (2002) Comparison of tibial plateau angle between clinically normal Greyhounds and Labrador retrievers with and without rupture of the cranial cruciate ligament. J Am Med Vet Assoc 221 (10), 1426-1429 PubMed.
Sandman K S, Harari J (2001) Canine cranial cruciate repair techniques; is one best? Vet Med 96 (11), 850-856 VetMedResource.
Geels J J, Roush J K, Hoskinson J J, McLaughlin R M (2000) Evaluation of an intracapsular technique for cranial cruciate ligament rupture: clinical, radiographic, scintigraphic and force plate analysis findings in 20 dogs. Vet Comp Orthop Traumatol 13 (4), 197-203 VetMedResource.
Kudnig ST (2000) Intra-articular replacement. Aust Vet J 78 (6), 384-385 PubMed.
Smith B (2000) Extracapsular stabilisation. Aust Vet J 78 (6), 382-383 PubMed.
Watt P (2000) Tibial plateau levelling. Aust Vet J 78 (6), 385-386 PubMed.
Chauvet A E et al (1996) Evaluation of fibular head transposition, lateral fabellar sutures and conservative treatment of cranial cruciate ligament injuries in large dogs: a retrospective study. J Am Anim Hosp Assoc 32 (3), 247-255 PubMed.
Anderson J (1994) The stifle. In: Manual of Small Animal Arthrology. Eds. J Houlton & R Collinson. Cheltenham: BSAVA, p 280.
Cranial cruciate ligament rupture. Schulz K. In Fossum TW (ed): Small Animal Surgery, 3rd ed-St. Louis: Mosby, 2007, pp 1254-1275.
Tibial tuberosity advancement (TTA): Early results in 63 dogs. Boudrieau RJ. Vet Comp Orthop Traumat 19:38(A), 2006.
Tibial tuberosity advancement for stabilisation of the canine cranial cruciate ligament-deficient stifle joint: Surgical technique, early results, and complications in 101 dogs. Lafever S, Miller NA, Stubbs WP, et al. Vet Surg 36:573-586, 2007.
Applications of evidence-based medicine: Cranial cruciate ligament injury repair in the dog. Aragon CL, Budsberg SC. Vet Surg 34:93-98, 2005.
Tibial osteotomies for cranial cruciate ligament insufficiency in dogs. Kim SE, Pozz A, Kowaleski MP, Lewis DD. Vet Surg 37:111-125, 2008.